The following case is a female is her twenties who was involved in a car accident. She presented with an isolated injury to the distal metaphysis of the humerus. She was diagnosed with a displaced closed fracture with significant gapping at the fracture side as demonstrated by the preoperative X-ray below. She had an intact radial nerve at presentation which is always of concern due to the anatomic location of the fracture. Studies show that the rate of radial nerve palsy with fractures at this location reaches between 11-23% of the cases. Of note, the radial nerve runs in the spiral groove of the distal 1/3 of the humerus and is endangered not only by the fracture but by the surgery as well.

CLICK IMAGES FOR LARGER VERSION.
Location of the radial nerve and proximity of the fracture.

Preoperative Xray demonstrates the distal spiral fracture.
The patient underwent an open reduction and internal fixation of the fracture using a 4.5mm narrow non locking compression plate along with placement of inter-fragment lag screws (3 x 3.5 mm screws).
The patient was positioned in lateral decubitus.
 |
| Picture from aofoundation.org |
The posterior approach was utilized with provides 55% exposure of the distal humerus without mobilization of the radial nerve and 75% humeral exposure when the radial nerve is mobilized. In any case, the RADIAL NERVE must be visualized and protected and more importantly the plate must BE VISUALIZED in its entire length when applied on the bone to avoid iatrogenic damage to the nerve. In this case the radial nerve was mobilized and protected.


Picture from aofoundation.org
 |
| Picture from aofoundation.org |
 |
| AP view after surgery and plating using 4.5mm plate and 3 lag screws |
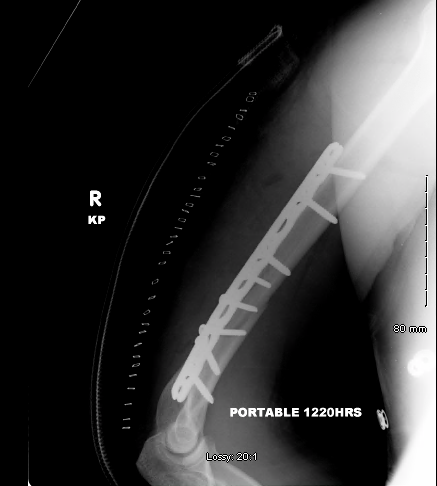 |
Lateral view after the placement of the plate |
5 months after surgery the fracture is completely healed as shown below.

Often times it seems that the appropriate fixation is stabilization of the fracture with eight cortices of fixation and a minimum of three to four screws inserted proximal and distal to the fracture.
It seems more accurate to take into consideration the concept of the working length of the plate. According to this concept increased fixation strength is noted with placement of screws close to the fracture, followed by plate fixation with screws spaced over a longer length plate. The working length of the plate may be more important than the number of cortices of fixation, and the increased spacing between screws provides advantages.
In the case described above three screws were spaced out proximally while fixation of the distal fragment was achieved with two plate screws and 3 inter-fragment lag screws.
A similar case which is more challenging is depicted below. The large butterfly fragment makes this fracture highly unstable and difficult to control rotationally. Placement of a mini plate or lag screws and conservation of the three part to a two part fracture may be necessary for control of the reduction and biomechanical stability of the fracture. The challenge with the segmental fractures at this level of the humerus is that the lag screws are difficult to be placed from lateral to medial direction as they may endanger the ulnar nerve. Mobilization of the ulnar nerve may be necessary. In addition, in muscular individuals, as in this case, the triceps splitting approach poses an obstacle to the placement of the lag screws as the bulk of the retracted medially or laterally triceps muscle (splitting approach) blocks or forces the screwdrivers or drills posteriorly. This "technical" limitation forces the trajectory of the lag screw in a rather oblique than parallel to the coronal plane direction on the bone. This is not ideal when the distal humerus is split in half on the sagittal plane as in this case. Remember that the humerus is flattened distally which makes lag screw placement more difficult as described above.





Further reading:
Management of Humeral Shaft Fractures
J Am Acad Orthop Surg July 2012 ; 20:423-433