
Today the term impingement is being used less frequently because it creates confusion to physicians and patients. With an MRI or with arthroscopy we can find out more about those conditions that were described as impingement in the past.
 |
| CLICK ON THE IMAGE FOR LARGER VERSION OF THE PICTURE |
.jpg) |
| CLICK ON THE IMAGE FOR LARGER VERSION OF THE PICTURE |
What about the bone spurs in my shoulder? Do these cause pain or rotator cuff tears?
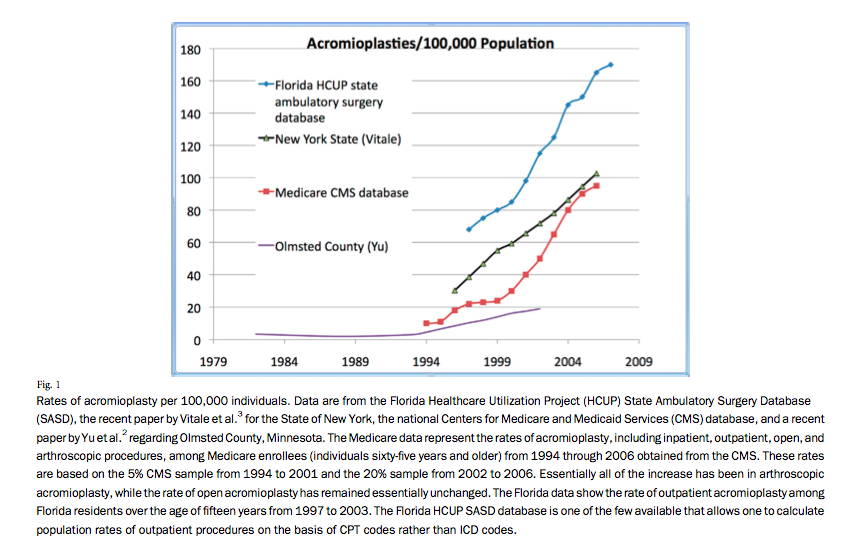
A lot of physicians will support the idea that a bone spur is the source of pain to your shoulder. It is important to recognize that sometimes the bone spurs can be painful. However, recent research has shown that a bone spur is not always the source of pain. The common mistake made in the diagnosis of shoulder conditions is that an MRI report or an Xray report with contain the wording "bone spur" and that will trigger an evaluation of the spurs for possible pain. It must be highlighted that the bone spurs are seen in multiple locations in our our joints. Knees, spine, heel bone for example. These bone spurs are not removed with the intent to treat your pain in these joints with the exception of the spine. In the spine they are removed only when they touch or compress a nerve. The bone spurs in the shoulder do not touch nerves. Today data shows that there is a high number of surgeons that do not believe that these shoulder spurs are the source of pain. They evaluate the shoulder carefully for the anatomic problem that causes the pain. They is a tremendous increase in the acromioplasties of the shoulder (shaving of bone spurs) that are performed in the US. This trend has changed over the past few years. The proof to that is that there are Level I studies (most accurate studies) that show that rotator cuff tendon repair without or with acromioplasty (removing the bone spurs) has the same result in the function of the shoulder.
Anatomy - What structures are involved in this condition?
Your shoulder is made up of three bones: your upper arm bone (humerus), your shoulder blade (scapula), and your collarbone (clavicle).
Your arm is kept in your shoulder socket by your rotator cuff. These muscles and tendons form a covering around the head of your upper arm bone and attach it to your shoulder blade.
There is a lubricating sac called a bursa between the rotator cuff and the bone on top of your shoulder (acromion). The bursa allows the rotator cuff tendons to glide freely when you move your arm. The bone spurs form on the undersurface of the acromion and come in contact with the rotator cuff naturally. Your doctor will explain to you if the spur is large enough to cause problems to the rotator cuff tendons.

Marked area is the "subacromial space" ie the space under the acromion where spurs can form. Today studies show that these spurs are infrequently associated with pain and most of the time the pain originates from the tendon that connects to the ball (humerus). Most commonly affected tendon is the supraspinatus as shown in this picture
Anatomy and description
The rotator cuff is a common source of pain in the shoulder. It is so common that the health care dollars spend for this condition are in the range of several billion dollars per year (single digit number). Pain can be the result of:
 |
| Normal MRI of the shoulder. Click on the image for larger size. |
- Tendinitis. The rotator cuff tendons can be irritated or damaged without disruption of the fibers of the tendon. This is called inflammation. It is seen on the MRI of the shoulder below. For better understanding and comparison a normal MRI is depicted as well.

Pathologic tendon - increased signal (white) where the arrow is indicates tendinitis - Bursitis. The bursa can become inflamed and swell with more fluid causing pain.

The bursa is the purple tissue, between the tendons and the acromion. In this picture a cortizone injection is given to treat the inflammed tissue - Impingement. As explained above this term is being used less frequently. We avoid using this term now because most of the time we can identify the source of pain. Doctors who still believe in the theory of impingement syndrome will explain to you that when you raise your arm to shoulder height, the space between the acromion and rotator cuff narrows. The acromion can rub against (or "impinge" on) the tendon and the bursa, causing irritation and pain. The problem with this theory is that 80-90% of the tendon tears start on the undersurface of the tendon which does not come in contact with the spur


Most patients will have pain from the rotator cuff as a result of inflammation or wear and tear of the tendon after the age of 40. If there is history of injury or overuse of the shoulder, like in young athletes and middle-aged people, use of the arms overhead for swimming, baseball, and tennis are particularly associated with this disease. Those who do repetitive perform lifting or overhead activities using the arm, such as paper hanging, construction, or painting are also susceptible.
Pain may also develop as the result of a minor injury. Sometimes, it occurs with no apparent cause.
Rotator cuff pain commonly causes local swelling and tenderness in the front of the shoulder. You may have pain and stiffness when you lift your arm. There may also be pain when the arm is lowered from an elevated position. At the beginning symptoms may be mild. Patients frequently do not seek treatment at an early stage. These symptoms may include:
- Minor pain that is present both with activity and at rest
- Pain radiating from the front of the shoulder to the side of the arm
- Sudden pain with lifting and reaching movements
- Athletes in overhead sports may have pain when throwing or serving a tennis ball
As the problem progresses, the symptoms increase:
- Pain at night
- Loss of strength and motion
- Difficulty doing activities that place the arm behind the back, such as buttoning or zippering
If the pain comes on suddenly, the shoulder may be severely tender. All movement may be limited and painful.
Your doctor will examine your shoulder for tenderness in any area and perform several tests with the arm in specific positions. He will evaluate the range of motion of your shoulder and test the strength of your arm.
A lot of patients go to the doctor for shoulder pain however the source of the problem is the neck and the shoulder hurts due to radiation of the pain from the neck to the shoulder (referred pain). The doctor will tell you if the neck is the origin of your problem.Do I have to have an MRI to see the problem?
The workup of your problem will start with plain X-rays to evaluate the bones. If you have no history of trauma, no loss of strength and no prior treatment to your shoulder it will be appropriate for your doctor to avoid an MRI and prescribe exercises for your shoulder. He will consider an MRI later on if the problem persists after a course of physical therapy or other type of conservative treatment.
Magnetic resonance imaging (MRI) and ultrasound. With these tests the doctor with be able to evaluate your tendons and ligaments. They can show fluid or inflammation in the bursa and rotator cuff. Please see pictures above.
How is this problem being treated today?
The doctor will select the best treatment for you based on several factors that he will take into consideration. These are your age, history of trauma, imaging findings, loss of strength or motion, prior treatments, smoking status, history of diabetes, functional level, sports activity, quality and quantity of the tendons that you have in your shoulder.
If I do not have surgery what kind of treatment will I need?
The doctor will select the best treatment for you based on several factors that he will take into consideration. These are your age, history of trauma, imaging findings, loss of strength or motion, prior treatments, smoking status, history of diabetes, functional level, sports activity, quality and quantity of the tendons that you have in your shoulder.
If I do not have surgery what kind of treatment will I need?
In most cases, the first line of treatment is nonsurgical. Although nonsurgical treatment may take several weeks to months, many patients experience a gradual improvement and return to function.
Rest. Your doctor may suggest rest and activity modification, such as avoiding overhead activities.Non-steroidal anti-inflammatory medicines. Drugs like ibuprofen and naproxen reduce pain and swelling.
Physical therapy and exercises. These can be done with a physical therapist or your can do those on your own under the guidance of your doctor. The first goal is to restore the range of motion to your shoulder. Stretching exercises are important for that reason.
Once your pain is improving and your range of motion, the next step will be on a strengthening program for the rotator cuff muscles.
Steroid injection. An injection of a mixture of cortizone with anesthetic pain medication is given mostly for diagnostic reasons and for short term relief of your pain. If you doctor injects the shoulder and you pain goes away depending on the anatomic location that the injection was given he or she will draw conclusions about the condition you have. You cannot have too many cortizone injections and most physicians will not give more than 4 in one year. These injections are given in 3 month intervals.
Surgical Treatment
For the surgical treatment of the rotator cuff tears and the rehabilitation protocol please refer to "Rotator Cuff Tears: Surgical Treatment Options" and "Physical Therapy programs" of this blog.
For a detailed explanation of new findings on the diagnosis of impingement syndrome please click here
Reference: http://www.ncbi.nlm.nih.gov/pubmed/22005869
Please also read the rheumatology network recommendation at: http://www.rheumatologynetwork.com/articles/redefine-shoulder-impingement-syndrome-enhanced-diagnosis
And here: http://www.mltj.org/materiale_cic/704_3_3/6089_impinge/article.htm
For a detailed explanation of new findings on the diagnosis of impingement syndrome please click here
Reference: http://www.ncbi.nlm.nih.gov/pubmed/22005869
Please also read the rheumatology network recommendation at: http://www.rheumatologynetwork.com/articles/redefine-shoulder-impingement-syndrome-enhanced-diagnosis
And here: http://www.mltj.org/materiale_cic/704_3_3/6089_impinge/article.htm